| ABC of clinical electrocardiography. Introduction. I—Leads, rate, rhythm, and cardiac axis. |
АВС клинической электрокардиографии.Введение. Отведения, частота, ритм и ось сердца. |
| Electrocardiography is a fundamental part of cardiovascular assessment. It is an essential tool for investigating cardiac arrhythmias and is also useful in diagnosing cardiac disorders such as myocardial infarction. Familiarity with the wide range of patterns seen in the electrocardiograms of normal subjects and an understanding of the effects of non-cardiac disorders on the trace are prerequisites to accurate interpretation. | ЭКГ – фундаментальная часть оценки сердечно-сосудистой системы. Это основной инструмент для исследования аритмий сердца, и является также полезным для диагностики сердечной патологии, такой как инфаркт миокарда. Знакомство с широким набором паттернов (вариантов), которые видны на ЭКГ здоровых людей, и понимание влияния некардиологических нарушений на запись ЭКГ, являются предпосылками для точной интерпретации. |
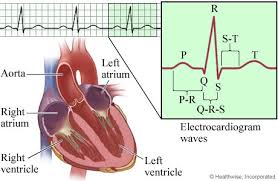
| The contraction and relaxation of cardiac muscle results from the depolarisation and repolarisation of myocardial cells. These electrical changes are recorded via electrodes placed on the limbs and chest wall and are transcribed on to graph paper to produce an electrocardiogram (commonly known as an ECG). |
Сокращение и расслабление миокарда происходят в результате деполяризации и реполяризации миоцитов. Данные электрические изменения записываются посредством электродов, размещенных на конечностях и грудной клетке, и передаются на миллиметровую бумагу, чтобы получилась электрокардиограмма (общеизвестная как ЭКГ). |
| The sinoatrial node acts as a natural pacemaker and initiates atrial depolarisation. The impulse is propagated to the ventricles by the atrioventricular node and spreads in a coordinated fashion throughout the ventricles via the specialised conducting tissue of the His-Purkinje system. Thus, after delay in the atrioventricular node, atrial contraction is followed by rapid and coordinated contraction of the ventricles. |
Синоатриальный узел действует как естественный водитель ритма и вызывает деполяризацию предсердий. Импульс передается к желудочкам посредством атрио-вентрикулярного узла и распространяется координированным образом по желудочкам через специализированную проводящую ткань системы Гиса-Пуркинье. Таким образом, после задержки в атриовентрикулярном узле за сокращением предсердий следует быстрое и координированное сокращение желудочков. |
| The electrocardiogram is recorded on to standard paper travelling at a rate of 25 mm/s. The paper is divided into large squares, each measuring 5 mm wide and equivalent to 0.2 s. Each large square is five small squares in width, and each small square is 1 mm wide and equivalent to 0.04 s. | ЭКГ записывается на стандартной бумаге, двигающейся со скоростью 25 мм/сек. Бумага разделена на большие квадраты, каждый 5 мм шириной, эквивалентный 0.2 сек. Каждый большой квадрат составляет 5 малых квадратов, а каждый малый квадрат составляет 1 мм и эквивалентен 0.04 сек. |
| The electrical activity detected by the electrocardiogram machine is measured in millivolts. Machines are calibrated so that a signal with an amplitude of 1 mV moves the recording stylus vertically 1 cm. Throughout this text, the amplitude of waveforms will be expressed as: 0.1 mV = 1 mm = 1 small square. |
Электрическая активность, определяемая электрокардиографом, измеряется в милливольтах. Аппараты калибруются, так чтобы сигнал с амплитудой 1 милливольт передвигает самописец вертикально на 1 см. В этой статье амплитуда волн будет выражаться как: 0.1 милливольт=1 мм=1 малый квадрат. |
| The amplitude of the waveform recorded in any lead maybe influenced by the myocardial mass, the net vector of depolarisation, the thickness and properties of the intervening tissues, and the distance between the electrode and the myocardium. Patients with ventricular hypertrophy have a relatively large myocardial mass and are therefore likely to have high amplitude waveforms. In the presence of pericardial fluid, pulmonary emphysema, or obesity, there is increased resistance to current flow, and thus waveform amplitude is reduced. |
На амплитуду сигнала, записанного в любом отведении, могут влиять масса миокарда, вектор деполяризации, толщина и свойства промежуточных тканей, а также расстояние между электродами и миокардом. Пациенты с гипертрофией желудочков имеют относительно большую массу миокарда, и вероятнее всего, будут иметь волны с большой амплитудой. При наличии перикардиальной жидкости, легочной эмфиземы, ожирения существует усиленное сопротивление электрическому току, поэтому амплитуда волн снижена. |
| The direction of the deflection on the electrocardiogram depends on whether the electrical impulse is travelling towards or away from a detecting electrode. By convention, an electrical impulse travelling directly towards the electrode produces a upright (“positive”) deflection relative to the isoelectric baseline, whereas an impulse moving directly away from an electrode produces a downward (“negative”) deflection relative to the baseline. When the wave of depolarisation is at right angles to the lead, an equiphasic deflection is produced. |
Направление зубца на ЭКГ зависит от того, движется ли электрический импульс в направлении к измеряющему электроду или от него. Условленно, что электрический импульс, идущий точно в направлении электрода (примечание: т.е. их направления совпадают), производит положительный относительно изоэлектрической линии зубец; в то время, как импульс, идущий точно в противоположном от электрода направлении, производит отрицательный относительно изолинии зубец. Когда волна деполяризации идет под прямым углом к отведению, формируется равнофазный зубец. |
| The six chest leads (V1 to V6) “view” the heart in the horizontal plane. The information from the limb electrodes is combined to produce the six limb leads (I, II, III, aVR, aVL, and aVF), which view the heart in the vertical plane. The information from these 12 leads is combined to form a standard electrocardiogram. |
Шесть грудных отведений (V1-V6) «обозревают» сердце в горизонтальной плоскости. Информация от электродов конечностей объединяется, чтобы образовать шесть отведений конечностей (I, II, III, aVR, aVL, и aVF), которые «обозревают» сердце в вертикальной плоскости. Информация от этих 12 отведений собирается и воспроизводит стандартную электрокардиограмму. |
 Документ можно скачать здесь:
Документ можно скачать здесь:
http://vk.com/doc207555293_411422504
0

